Apart from clinical care, what broad themes of quality general practice should be considered when responding to a registrar in Nicole’s situation?
What does the registrar need to learn?
Learners will come with learning needs – mainly those they want to learn. These are driven by identified knowledge and skill gaps, and exams…
But there are many things they need to learn.
The RACGP uses the star analogy to describe general practice through 5 domains of general practice: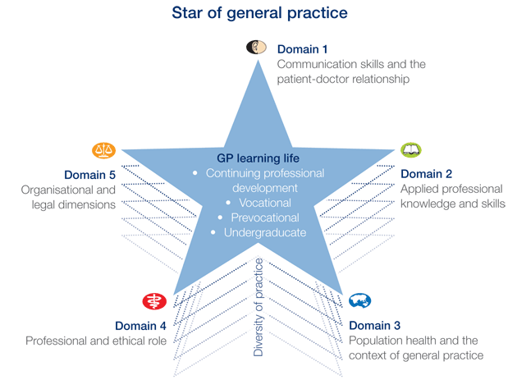
How would you help Nicole address the Unknown Unknowns in this scenario?
Teaching the registrar about uncertainty in the context of Long COVID
- Accept that uncertainty is inevitable
- Gather sufficient data
- Identify the patient’s agenda
- Reason analytically
- Share decision-making
- Seek evidence
- Safety net


Why is Nicole asking for help?
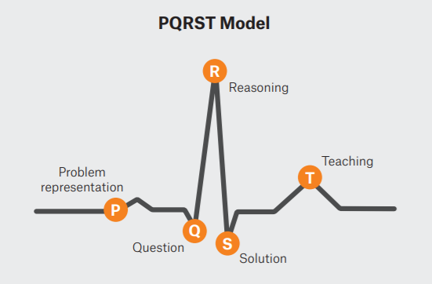
How can the PQRST framework be used here?

What resources would you first point Nicole to?
Date reviewed: 15 April 2025
Please note that while reasonable care is taken to provide accurate information at the time of creation, we frequently update content and links as needed. If you identify any inconsistencies or broken links, please let us know by email.
This website uses cookies. Read our privacy policy.