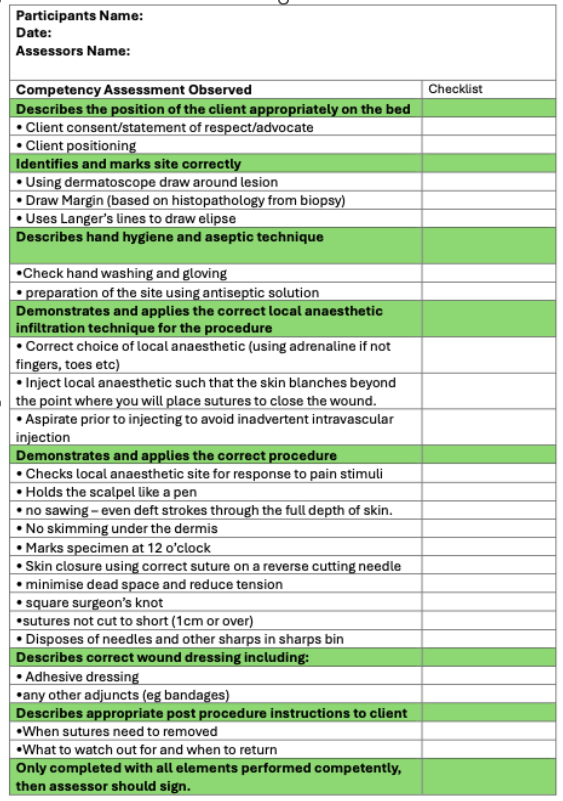
WHAT IS A COMPETENCY CHECK LIST?
A competency checklist lists all the key steps and can be used as an assessment tool. For example,
HOW DO I STRUCTURE PROCEDURAL SKILL TEACHING FOR REGISTRARS?
HOW DO I MANAGE THE COGNITIVE LOAD FOR LEARNERS?
HOW DO I KNOW IF MY REGISTRAR IS READY TO PERFORM A PROCEDURE INDEPENDENTLY?
WHAT IS "DELIBERATE PRACTICE" AND WHY IS IT IMPORTANT?
WHAT IF MY REGISTRAR LACKS CONFIDENCE OR REFUSES TO DO CERTAIN PROCEDURES?
HOW DO I INCLUDE PATIENT-CENTRED CARE IN PROCEDURAL TRAINING?
HOW DO I TEACH IF I’VE LOST CONFIDENCE IN A SKILL MYSELF?
ARE ALL PROCEDURES SUITABLE FOR THIS APPROACH?
WHAT TOOLS OR RESOURCES CAN I USE TO SUPPORT THIS?
WHAT IS A FINAL TIP FOR SUPERVISORS?
REFERENCES

Date reviewed: 02 February 2026
Please note that while reasonable care is taken to provide accurate information at the time of creation, we frequently update content and links as needed. If you identify any inconsistencies or broken links, please let us know by email.
This website uses cookies. Read our privacy policy.