Learners will come with learning needs – mainly those they want to learn. These are driven by identified knowledge and skill gaps, and exams…
But there are many things they need to learn.
The RACGP uses the star analogy to describe general practice through 5 domains of general practice: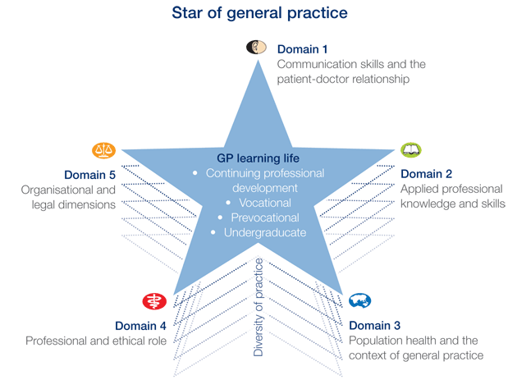



Date reviewed: 02 October 2023
Please note that while reasonable care is taken to provide accurate information at the time of creation, we frequently update content and links as needed. If you identify any inconsistencies or broken links, please let us know by email.
GPTA Ltd t/as GP Supervision Australia
PO Box 787 Gisborne Vic 3437
Level 40/140 William Street Melbourne Vic 3000
